Fatty liver disease is now one of the most common chronic liver conditions worldwide, affecting an estimated 1 in 3 adults. Often silent in its early stages, it can progress over time to liver inflammation, scarring, and even cirrhosis if left unaddressed.
Previously known as non-alcoholic fatty liver disease (NAFLD), the condition is now more accurately referred to as Metabolic Associated Steatotic Liver Disease (MASLD). This updated terminology reflects what research has made clear: fatty liver is not just a liver problem, but a systemic metabolic condition (1). The encouraging news is that fatty liver is largely preventable and often reversible, especially when identified early. Nutrition, physical activity, sleep, and metabolic health play a central role in both prevention and treatment.
Understanding Fatty Liver Disease
Fatty liver develops when excess fat accumulates inside liver cells (hepatocytes). In its simplest form, this is called simple steatosis and is often reversible.
In some individuals, however, fatty liver progresses to metabolic dysfunction-associated steatohepatitis (MASH), where fat accumulation is accompanied by inflammation and liver cell injury. Over time, ongoing injury may lead to fibrosis (scar tissue), cirrhosis, and in some cases hepatocellular carcinoma (liver cancer) (2).
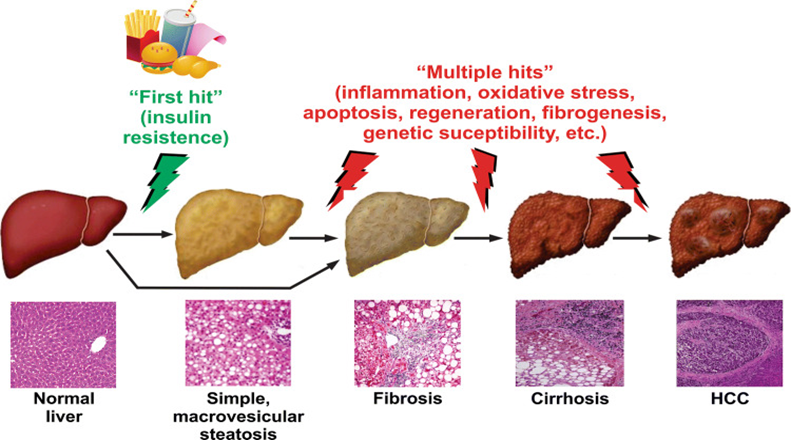
Figure 1: Progression of fatty liver disease. Insulin resistance leads to fat accumulation in the liver (“first hit”), while ongoing metabolic, inflammatory, and oxidative stresses (“multiple hits”) drive progression from simple fatty liver to fibrosis, cirrhosis, and, in some cases, liver cancer (2)
The “First Hit” and “Multiple Hits” Model
Early research described fatty liver progression using a two-hit theory:
- Fat accumulation in the liver
- Oxidative stress and inflammation leading to liver damage
While helpful initially, this model is now considered oversimplified. Current evidence supports a “multiple hit” model, in which several processes occur simultaneously.
The First Hit: Insulin Resistance
The earliest driver of fatty liver is often insulin resistance, commonly associated with overweight, obesity, type 2 diabetes, and metabolic syndrome. When insulin signalling is impaired:
- More fat is delivered to the liver from adipose tissue
- The liver increases its own fat production
- Fat accumulates inside liver cells
At this stage, inflammation and scarring are minimal, and lifestyle interventions can be highly effective.
Multiple Hits Driving Progression
Progression occurs when fat accumulation is accompanied by:
- Chronic low-grade inflammation
- Oxidative stress
- Mitochondrial dysfunction (impaired energy production)
- Altered gut microbiota and increased intestinal permeability
- Genetic susceptibility
These overlapping “hits” explain why many people with fatty liver never develop advanced disease, while others progress despite similar body weight or lifestyle factors (3).
What Causes Fatty Liver?
The liver plays a central role in fat and carbohydrate metabolism. Fatty liver develops when this balance is disrupted.
Key contributors include:
- Excess caloric intake, especially from refined carbohydrates and added sugars (4)
- Insulin resistance, which impairs fat metabolism (4)
- High fructose intake, particularly from sugary drinks (4)
- Inflammation and oxidative stress within liver cells (4)
- Genetic factors, including variants in PNPLA3, TM6SF2, and MBOAT7 (5)
- Sedentary lifestyle and poor sleep quality
Although strongly associated with obesity, lean individuals can also develop fatty liver, particularly in the presence of insulin resistance or genetic risk (6).
Who Is Most at Risk?
Fatty liver can affect anyone, but the risk is higher among :
- Adults with overweight or obesity
- Individuals with type 2 diabetes or metabolic syndrome
- People consuming high amounts of added sugar or ultra-processed foods
- Those with a family history of liver disease
- Individuals with chronic sleep deprivation or high stress
- People taking certain medications (e.g., corticosteroids) (7),(8),(9)
Diet and Lifestyle Interventions That Work
Lifestyle modification is the first line and most effective treatment for fatty liver disease.

1. Gradual, Sustainable Weight Loss
- A 5–10% reduction in body weight can significantly reduce liver fat and inflammation
- Weight loss of ≥7–10% is associated with improvement or resolution of MASH in many individuals (10)
- Rapid or extreme dieting should be avoided, as it may worsen liver stress (11)

2. A Liver-Friendly Dietary Pattern
Strong evidence supports a Mediterranean-style diet, rich in:
- Vegetables, fruits, and legumes
- Whole grains and dietary fibre
- Nuts, seeds, and olive oil
- Fish and omega-3 fatty acids
Key dietary strategies include:
- Limiting added sugars, especially fructose from fizzy drinks, fruit juices, and sweets
- Reducing saturated and trans fats
- Ensuring adequate protein intake to support metabolic health and lean mass
Importantly, studies show that the Mediterranean diet can reduce liver fat even without significant weight loss, highlighting the importance of diet quality (12).

3. Regular Physical Activity
Exercise improves liver fat content independently of weight loss.
- Aerobic exercise reduces liver fat and improves cardiovascular health
- Resistance training enhances insulin sensitivity and muscle mass
- Aim for 150–200 minutes per week of moderate-intensity activity
Combining both aerobic and resistance training gives the greatest metabolic benefit (4).

4. Sleep and Stress Management
Emerging evidence links poor sleep and chronic stress with insulin resistance and fatty liver progression (13).
- Aim for 7–9 hours of quality sleep per night
- Address sleep apnoea when present
- Incorporate stress-reduction practices such as mindfulness, yoga, or breathing exercises

5. Alcohol Intake
Even moderate alcohol consumption may worsen liver injury in people with fatty liver.
For those with MASLD or MASH, minimising or avoiding alcohol is generally recommended (14).
Emerging Areas in Fatty Liver Research

1. The Gut–Liver Axis
The liver receives most of its blood supply from the gut, making gut health a key regulator of liver inflammation (15).
- Dysbiosis and increased intestinal permeability allow bacterial products to reach the liver
- Fibre-rich diets, prebiotics, and probiotics may improve liver fat and inflammation
- This reinforces the importance of dietary diversity and whole foods
2. Genetics and Personalised Risk
Genetic variants influence susceptibility and disease progression, helping explain:
- Fatty liver in lean individuals
- Variable progression among people with similar lifestyles
Future approaches may combine genetics with lifestyle interventions for personalised care (5).
3. Hormones, Adipose Tissue, and Systemic Inflammation
Fatty liver is increasingly recognised as a disease of whole-body metabolic dysfunction (16):
- Dysfunctional fat tissue releases inflammatory signals
- Insulin resistance in muscle and adipose tissue worsens liver fat accumulation
- Resistance training and muscle preservation are, therefore, critical components of therapy

4. Medications and Supplements
While no medication replaces lifestyle intervention:
- GLP-1 receptor agonists show promise in reducing liver fat, largely via metabolic effects (17)
- Vitamin E may benefit select non-diabetic adults with MASH under medical supervision (18)
- Anti-fibrotic therapies are under active investigation

Signs, Diagnosis, and Screening
Fatty liver is often asymptomatic. When present, symptoms may include:
- Fatigue
- Mild discomfort in the upper right abdomen
Screening tools include:
- Liver enzymes (ALT, AST)
- Ultrasound or transient elastography
- Risk scores combining metabolic and clinical markers
Early detection allows timely intervention and prevents progression (1).
Key Takeaways
- Fatty liver disease is common but often reversible
- It is driven by metabolic dysfunction rather than alcohol alone
- Effective strategies include:
- Sustainable weight management
- Mediterranean-style eating
- Regular physical activity
- Adequate sleep and stress management
- Minimising added sugar and alcohol
- Genetics and gut health influence risk and progression
- Early screening is essential for the prevention of advanced disease
5 Steps to Support Liver Health Naturally
- Eat a whole-food, Mediterranean-style diet
- Exercise regularly (aerobic + resistance training)
- Maintain healthy, gradual weight loss if needed
- Prioritise sleep and stress management
- Limit or avoid alcohol
Final Note
Lifestyle interventions remain the cornerstone of fatty liver management. Individuals with suspected advanced disease or persistently abnormal liver tests should work closely with a qualified healthcare professional.
References
1. Al Hashmi K, Giglio RV, Pantea Stoian A, Patti AM, Al Waili K, Al Rasadi K, et al. Metabolic dysfunction-associated fatty liver disease: current therapeutic strategies. Front Nutr. 2024 Mar 19;11:1355732.
2. Friedman SL, Neuschwander-Tetri BA, Rinella M, Sanyal AJ. Mechanisms of NAFLD development and therapeutic strategies. Nat Med [Internet]. 2018 Jul 1 [cited 2026 Jan 31];24(7):908. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC6553468/
3. Bessone F, Razori MV, Roma MG. Molecular pathways of nonalcoholic fatty liver disease development and progression. Cell Mol Life Sci [Internet]. 2018 Jan 15 [cited 2026 Jan 31];76(1):99. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC11105781/
4. Romero-Gómez M, Zelber-Sagi S, Trenell M. Treatment of NAFLD with diet, physical activity and exercise. J Hepatol [Internet]. 2017 Oct 1 [cited 2026 Jan 31];67(4):829–46. Available from: https://www.journal-of-hepatology.eu/action/showFullText?pii=S0168827817320524
5. Juanola O, Martínez-López S, Francés R, Gómez-Hurtado I. Non-Alcoholic Fatty Liver Disease: Metabolic, Genetic, Epigenetic and Environmental Risk Factors. Int J Environ Res Public Health [Internet]. 2021 May 2 [cited 2026 Jan 31];18(10):5227. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC8155932/
6. Younossi ZM. The Epidemiology of Nonalcoholic Steatohepatitis An Official Learning Resource of AASLD. 2018 [cited 2026 Jan 31];11. Available from: http://liverlearning.aasld.org/aasld/2017/thelivermeeting/195652/
7. Pouwels S, Sakran N, Graham Y, Leal A, Pintar T, Yang W, et al. Non-alcoholic fatty liver disease (NAFLD): a review of pathophysiology, clinical management and effects of weight loss. BMC Endocr Disord [Internet]. 2022 Dec 1 [cited 2026 Jan 31];22(1):63. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC8919523/
8. Bu LF, Xiong CY, Zhong JY, Xiong Y, Li DM, Hong FF, et al. Non-alcoholic fatty liver disease and sleep disorders. World J Hepatol [Internet]. 2024 [cited 2026 Jan 31];16(3):304. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC10989311/
9. Nonalcoholic Fatty Liver. LiverTox: Clinical and Research Information on Drug-Induced Liver Injury [Internet]. 2019 May 4 [cited 2026 Jan 31]; Available from: https://www.ncbi.nlm.nih.gov/books/NBK547860/
10. Brunner KT, Henneberg CJ, Wilechansky RM, Long MT. Nonalcoholic Fatty Liver Disease and Obesity Treatment. Curr Obes Rep [Internet]. 2019 Sep 15 [cited 2026 Jan 31];8(3):220. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC6770992/
11. Rinella ME, Neuschwander-Tetri BA, Siddiqui MS, Abdelmalek MF, Caldwell S, Barb D, et al. AASLD Practice Guidance on the clinical assessment and management of nonalcoholic fatty liver disease. Hepatology [Internet]. 2023 May 1 [cited 2026 Jan 31];77(5):1797–835. Available from: https://journals.lww.com/hep/fulltext/2023/05000/aasld_practice_guidance_on_the_clinical_assessment.31.aspx
12. Ryan MC, Itsiopoulos C, Thodis T, Ward G, Trost N, Hofferberth S, et al. The Mediterranean diet improves hepatic steatosis and insulin sensitivity in individuals with non-alcoholic fatty liver disease. J Hepatol [Internet]. 2013 Jul 1 [cited 2026 Jan 31];59(1):138–43. Available from: https://www.journal-of-hepatology.eu/action/showFullText?pii=S0168827813001347
13. Yang J, Zhang K, Xi Z, Ma Y, Shao C, Wang W, et al. Short sleep duration and the risk of nonalcoholic fatty liver disease/metabolic associated fatty liver disease: a systematic review and meta-analysis. Sleep Breath [Internet]. 2022 Oct 1 [cited 2026 Jan 31];27(5):1. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC9771780/
14. Marti-Aguado D, Calleja JL, Vilar-Gomez E, Iruzubieta P, Rodríguez-Duque JC, Del Barrio M, et al. Low-to-moderate alcohol consumption is associated with increased fibrosis in individuals with metabolic dysfunction-associated steatotic liver disease. J Hepatol [Internet]. 2024 Dec 1 [cited 2026 Jan 31];81(6):930–40. Available from: https://pubmed.ncbi.nlm.nih.gov/38971533/
15. Tilg H, Adolph TE, Trauner M. Gut-liver axis: Pathophysiological concepts and clinical implications. Cell Metab [Internet]. 2022 Nov 1 [cited 2026 Jan 31];34(11):1700–18. Available from: https://pubmed.ncbi.nlm.nih.gov/36208625/
16. Jung UJ, Choi MS. Obesity and Its Metabolic Complications: The Role of Adipokines and the Relationship between Obesity, Inflammation, Insulin Resistance, Dyslipidemia and Nonalcoholic Fatty Liver Disease. Int J Mol Sci [Internet]. 2014 Apr 11 [cited 2026 Jan 31];15(4):6184. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC4013623/
17. Semaglutide for the treatment of metabolic dysfunction-associated steatohepatitis – American College of Gastroenterology [Internet]. [cited 2026 Jan 31]. Available from: https://gi.org/journals-publications/ebgi/kwo_sep2025/
18. Sanyal AJ, Chalasani N, Kowdley K V, McCullough A, Diehl AM, Bass NM, et al. Pioglitazone, Vitamin E, or Placebo for Nonalcoholic Steatohepatitis. N Engl J Med [Internet]. 2010 May 6 [cited 2026 Jan 31];362(18):1675. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC2928471/
